
Employment-Based Health Insurance-Yes, It's Still A Thing

Two years ago I was betting that workplace health insurance was on its way out. I predicted that by the end of the decade at least one large employer would decide to get out of the health insurance sponsoring business (I was thinking IBM since they are not afraid of eliminating benefits). And, because employers generally play follow-the-leader employee benefit management games, I assumed the dominoes would fall.
Two years later, I see employers holding on for dear life to their employee benefit programs out of what I suspect is both fear and self-interest, and maybe some concern for the welfare of their employees. They know that employees prefer to have their benefit plans spoon-fed, and the tax savings don’t hurt either. But what I don’t understand is why employers are not trying to extract any positives from this historic health care reform moment.
Health care technology entrepreneurs are creating businesses to take advantage of the bounty that is health care reform. Health insurance brokers are courting individuals and enjoying record-breaking business growth. Big Pharma and hospitals are enjoying record profits. Insurance companies are creating wealth for their investors. And medical doctors are enjoying their status as the highest paid profession in America.
And employers…? Well, they are acting like business as usual in administering their health insurance plans. Continue Reading...
Medicare For All Could Save Life And Limb
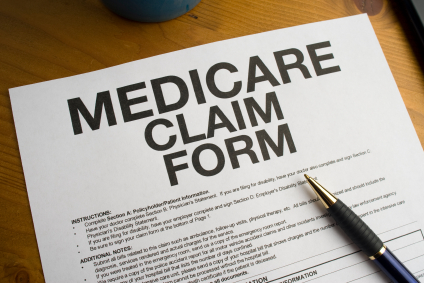
I recently heard a story of a diabetic Medicaid patient that developed gangrene on her foot and leg. Gangrene occurs when tissue decays or dies due to a loss of its blood supply or because of a bacterial infection. It's a concern for many people with diabetes because of how diabetes affects the body--including possible damage to the nerves and weakening of the immune system. Treatments for gangrene include surgical removal of the decaying or dead skin, amputation of the affected body part or antibiotics.
The first surgeon that examined the diabetic Medicaid patient's foot and leg concluded that amputation of the affected area was the appropriate course of care given the severity of the gangrene. He immediately scheduled surgery for later that day. Fortunately a second surgeon disagreed—concluding that the gangrene could be treated with surgical removal of the dead and dying skin. The surgery to remove the dead skin was performed by the second surgeon and the patient still has all of her limbs and is being monitored.
I won’t speculate why the first surgeon prescribed amputation to treat the gangrene, but I did wonder if the patient’s insurance coverage had anything to do with his rush to cut. And there is evidence to back up my worries. There is lots of evidence that diabetic amputees are more like to be poor and minority. Or course, this is not entirely the fault of doctors. Many poor minorities don’t seek regular or preventive care to treat their diabetes, making some amputations necessary. But not all of them…
And there’s more… A disease management program designed to help minority diabetes patients revealed the difference in blood testing rates between whites and ethnic minorities. Blacks and Hispanics had lower testing (to determine how well their diabetes is being controlled) rates than whites. A study of this vendor-based disease management pilot program for Medicare patients concluded that it did “not appear to improve diabetes care or mitigate racial/ethnic disparities among these patients…” The program failed.
But what’s a problem without a solution? Fortunately, health care reform is already addressing the diabetes crisis. A pilot diabetes prevention program run by the YMCA received praise and dollars from a grant program established by the Affordable Care Act program. According to an article on npr.org,
It's the first prevention program to meet requirements under the Affordable Care Act to gain Medicare coverage, HHS says, including undergoing an independent audit to confirm that it's effective and saves money. The Obama administration is recommending that Medicare cover the program for at-risk Medicare beneficiaries. Continue Reading...
It’s Not Skepticism Or Caution That Keeps Us From Upending Our Bloated Health Care System, It’s Unwillingness

Democratic presidential candidate, Bernie Sanders, relentlessly scoffs at the idea that Wall Street is Too Big To Fail. But it is his proposal to provide Medicare For All that exposes the real industry that is, in many people’s mind, Too Big To Fail—health care. A recent
Washington Post article all but admits this and the Post is not alone in its thinking.Throughout this very long campaign cycle countless politicians, policy wonks, economists, writers and everyday people have characterized Medicare For All as unrealistic or in Hillary Clinton’s recent words, “…too good to be true...” Seriously, how many euphemisms can opponents use to say what they’re really thinking—the health care industry is such a big part of our economy that we can’t change it. They are, however, right about health care being a large part of the U.S. economy in terms of money and jobs.
- Health care expenditures make up 17.5% of the nations gross domestic product (GDP). That means it is basically about 20% of the entire U.S. economy
- We spent a little over $3 trillion for health care in 2014
- The health care industry employs over 13 million workers and is the largest private sector business sector
It’s one thing to be concerned about the impact on the economy if the health care industry undergoes a major overhaul overnight, it’s another to think we should take a break from addressing health care’s growing affordability issues. However, it seems that every proposed change to make our health care system more transparent, accountable and affordable is met with excuses or snark.
Electronic Health Records (EHR) – too expensive to purchase; time-consuming to evaluate and implement; have privacy and system compatibility issues; lack protections for proprietary information
Drug Price Controls – stifle innovation; scare away investors; halt production
Price Transparency – ignores quality standards; too difficult to determine; ignores geographical price differences; limited number of shoppable services to make a difference
Mission Accomplished… Continue Reading...
Can You Purchase Prescription Medication From Abroad Like Maria Sharapova?

I’m a big fan of professional tennis. Like many tennis fans this week I was eager to hear the scheduled announcement on Monday by one of the biggest stars in the game, Maria Sharapova. Here announcement that she failed a mandatory drug test at the first tennis major of the year, the Australian Open, was a disappointing surprise. Maria admitted taking a drug since 2006 that was just recently banned (January 1, 2016) by the World Anti-Doping Agency (WADA).
The drug is called meldonium (aka mildronate) and the U.S. Food and Drug Administration (FDA) does not approve it—which mean it is not available by prescription in the U.S. But Maria is not an American citizen. She’s a Russian citizen who received her tennis training in the U.S. as a young child and owns several homes here. According to her announcement about the incident, her family physician prescribed meldonium to her to address several health issues.
The questions everyone’s asking now are:
- Where is her physician’s practice based?
- Where does she get the drug?
- Does she import the drug from a country where it is legal to the U.S.?
- Has the drug ever been administered to her in the U.S. in the ten (10 years) she’s been using it?
- Did she notify the FDA she was importing the drug and as a non-citizen did she have to?
- if the intended use is for a serious condition for which effective treatment may not be available domestically
- if the product is not considered to represent an unreasonable risk
- if the individual seeking to import the drug affirms in writing that it is for the patient's own use and provides the name and address of the U.S.-licensed doctor responsible for his or her treatment with the drug or provides evidence that the drug is for continuation of a treatment begun in a foreign country
- if the product is for personal use and is a three-month supply or less and not for resale, since larger amounts would lend themselves to commercialization
- if there is no known commercialization or promotion to U.S. residents by those involved in distribution of the product
We Need More Drug Importation Ban Exceptions Continue Reading...
Big Pharma Wants You To Believe Its Pricing Strategy Is About Aid For the Poor. Yeah, Right!

Never have I read an article and had such a strong negative reaction to it like
Caroline Chen's article on Bloomberg.com about Gilead Sciences drug pricing practices. This article is revelatory and maddening. It was a revelation (to me) because it's the first article I've read where Big Pharma shares how and why it decides to sell its drugs at vastly different prices worldwide. Like charging American hepatitis C sufferers $84,000 for Sovaldi and the Egyptians, $900... And, two, it reveals the impenetrable self-righteousness of Big Pharma.Just Who Do They Think They Are?
It takes (blank) for Gilead to present its strategy of charging outrageous drug prices to rich countries as the best way to help poor countries afford its products. As if lowering the price of the drug for everyone was not an option. But it's Gilead's attempt to paint itself as a good corporate citizen for working with poor nations that is most appalling. Because it's not true...
In Chen's article, Gilead presents itself as willingly entering into agreements with poor countries and charging them between 1% to 10% of what it charges the U.S. What Gilead leaves out is that this "strategy" was a preemptive strike to prevent these countries from making their own generic version of the drug. An Indian generics maker was already in the process of lobbying the Indian government for a license to make an affordable generic version of Sovaldi.
In fact this Sovaldi price issue is just another case of déjà vu all over again. It was pressure from poor countries and their advocates that made Big Pharma agree to $1 per pill HIV AIDS drugs decades ago. And it was pressure from the Egyptian and Indian governments that led to $900 hepatitis C treatment (cure) versus $84,000...
This Is Not Over Continue Reading...
 Denise Perkins
Denise Perkins




